What Are Ear Tubes?
Painful ear infections are a rite of passage for children – by the age of five, nearly every child has experienced at least one episode. Most ear infections either resolve on their own (viral) or are effectively treated by antibiotics (bacterial). But sometimes, ear infections and/or fluid in the middle ear may become a chronic problem, leading to other issues such as hearing loss, behavior, and speech problems. In these cases, insertion of an ear tube by an otolaryngologist may be considered.
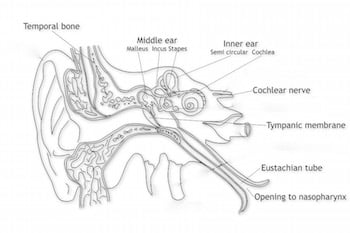
Ear tubes are tiny cylinders placed through the eardrum (tympanic membrane) to allow air into the middle ear. They may also be called tympanostomy tubes, myringotomy tubes, ventilation tubes, or PE (pressure equalization) tubes. These tubes can be made out of plastic, metal, or Teflon and may have a coating intended to reduce the possibility of infection. There are two basic types of ear tubes: short-term and long-term. Short-term tubes are smaller and typically stay in place for six months to a year before falling out on their own. Long-term tubes are larger and have flanges that secure them in place for a longer period of time. Long-term tubes may fall out on their own, but removal by an otolaryngologist is often necessary.
Who Needs Ear Tubes?
Ear tubes are often recommended when a person experiences repeated middle ear infection (acute otitis media) or has hearing loss caused by the persistent presence of middle ear fluid (otitis media with effusion). These conditions most commonly occur in children, but can also be present in teens and adults and can lead to speech and balance problems, hearing loss, or changes in the structure of the eardrum. Other less common conditions that may warrant the placement of ear tubes are malformation of the ear drum or Eustachian Tube, Down Syndrome, cleft palate, and barotrauma (injury to the middle ear caused by a reduction of air pressure), usually seen with altitude changes such as flying and scuba diving.
Each year, more than half a million ear tube surgeries are performed on children, making it the most common childhood surgery performed with anesthesia. The average age of ear tube insertion is one to three years old. Inserting ear tubes may:
- Reduce the risk of future ear infection
- Restore hearing loss caused by middle ear fluid
- Improve speech problems and balance problems
- Improve behavior and sleep problems caused by chronic ear infections
How Are Ear Tubes Inserted?
During an outpatient surgical procedure, ear tubes are inserted through an incision called a myringotomy. A myringotomy refers to an opening created in the eardrum or tympanic membrane. This is most often done under a surgical microscope with a small scalpel. If an ear tube is not inserted, the hole would heal and close within a few days. To prevent this, an ear tube is placed in the hole to keep it open and allow air to reach the middle ear space.

Ear Tube Surgery
A myringotomy is performed and the fluid behind the eardrum (in the middle ear space) is suctioned out. The ear tube is then placed in the hole. Ear drops are administered after the ear tube is placed and may be necessary for a few days. The procedure usually lasts less than 15 minutes and patients awaken quickly. Sometimes the otolaryngologist will recommend removal of the adenoid tissue (lymph tissue located in the upper airway behind the nose) when ear tubes are placed. This is often considered when a repeat tube insertion is necessary. Current research indicates that removing adenoid tissue concurrent with the placement of ear tubes can reduce the risk of recurrent ear infections and the need for repeat surgery.
What To Expect After Surgery
After surgery, the patient is monitored in the recovery room and will usually go home within an hour. Patients usually experience little or no postoperative pain. Hearing loss caused by the presence of middle ear fluid is immediately resolved by surgery. The otolaryngologist will provide specific postoperative instructions for each patient, including when to seek immediate attention and follow-up appointments. He or she may also prescribe antibiotic ear drops for a few days.
Recent research suggests that protecting the ear may not be necessary, except when diving or engaging in water activities in unclean wate,r such as lakes and rivers. Parents should consult with the treating physician about ear protection after surgery.
Possible Complications
Myringotomy with insertion of ear tubes is an extremely common and safe procedure with minimal complications. When complications do occur, they may include:
- Perforation – This can happen when a tube comes out or a long-term tube is removed and the hole in the tympanic membrane (eardrum) does not close. The hole can be patched through a minor surgical procedure called a tympanoplasty or myringoplasty.
- Scarring – Any irritation of the eardrum (recurrent ear infections), including repeated insertion of ear tubes, can cause scarring called tympanosclerosis or myringosclerosis. In most cases, this causes no problems with hearing.
- Infection – Ear infections can still occur in the middle ear or around the ear tube. However, these infections are usually less frequent, result in less hearing loss, and are easier to treat – often only with ear drops. Sometimes an oral antibiotic is still needed.
- Ear Tubes Come Out Too Early Or Stay In Too Long – If an ear tube expels from the eardrum too soon (which is unpredictable), fluid may return and repeat surgery may be needed. Ear tubes that remain too long may result in perforation or may require removal by the otolaryngologist.
Consultation with an otolaryngologist (ear, nose, and throat surgeon) may be warranted if you or your child has experienced repeated or severe ear infections, ear infections that are not resolved with antibiotics, hearing loss due to fluid in the middle ear, barotrauma, or have an anatomic abnormality that inhibits the drainage of the middle ear.
Other Factors to Consider
Especially in adults, most ear infections do not occur as an isolated medical problem. There may be obstructive swelling in the nose or in the throat anatomy behind the nose, called the nasopharynx. Such swelling can cause obstruction or inhibit the function of the Eustachian Tube which is necessary to maintain normal ear function. Repeated administration of antibiotics for ear infections without a careful examination and initiation of appropriate treatment for conditions in the nasopharynx is unwise and should not be recommended without careful evaluation by an ear, nose, and throat specialist. Frequently, the annoying and destructive process of repeated ear infections can be arrested with the use of less troublesome nasal treatments.
Frequently Asked Questions about Ear Tubes
Are ear tubes really necessary?
Can an ear tube become dislodged?
Can ear tubes get clogged?
Can ear tubes improve hearing?
Can you fly after getting tubes in ears?
Can you get ear infection with tubes?
Can you swim with tubes in your ears?
Can your eardrum burst with tubes?
Do ear tubes hurt when they fall out?
Do ear tubes improve speech?
Do ears hurt after tubes?
How do ear tubes come out?
How do you know when tubes fall out of ears?
How do you wash your hair with tubes in your ears?
How long do tubes stay in your ears?
How will my child feel after ear tube surgery?
Is ear tube surgery painful for adults?
Is there pain after ear tube surgery?
What are the risks of ear tube surgery?
What do ear tubes look like?
What happens when tubes fall out of ears?
Who performs ear tube surgery?